

ß thalassaemia results from deletions in the ß globin gene. A normal human has 2 ß globin genes. Deletions in ß genes result in imbalanced synthesis of α globins and ß globins. As a result, excess free α globin chains accumulate and precipitate in red cell precursors, interfering with maturation and resulting in intramedullary destruction of erythroid precursors. This is known as ineffective erythropoiesis. The RBCs that enter the circulating contain varying amounts of free α globin (the amount increases with the phenotypic severity of the ß thalassaemia). The α globin and its breakdown products are deleterious to the red cell membrane, causing it to become more rigid and resulting in shortened red cell survival.
A high RBC count with a microcytic anaemia is typical of the ineffective erythropoiesis and shortened red cell survival in ß thalassaemia.
ß thalassaemia mutations are common in the Mediterranean, India, Southeast Asia. They can occasionally be seen in Afro-Caribbeans.
Patients with ß thalassaemia trait have a mild anaemia (Hb usually 100-110g/L) with microcytosis.


Blood film features:
- Mild anaemia
- Microcytic, hypochromic
- Occasional target cells
- Anisopoikilocytosis range from marked to mild
- Basophilic stippling
- Polychromasia
Differential diagnosis:
- Iron deficiency (more elliptocytes, haemoglobin in cells may be less evenly distributed, polychromasia less common, RBC count low).
- Co-existing iron deficiency and thalassaemia trait
- Sideroblastic anaemia (usually dimorphic picture).
- Congenital dyserythropoietic anaemia (normocytic with macrocytes).
Haemoglobin electrophoresis:

Alkaline gel electrophoresis from a patient with ß thalassaemia trait. There are no abnormal bands. The acid gel is also normal in ß thalssaemia trait
HPLC:
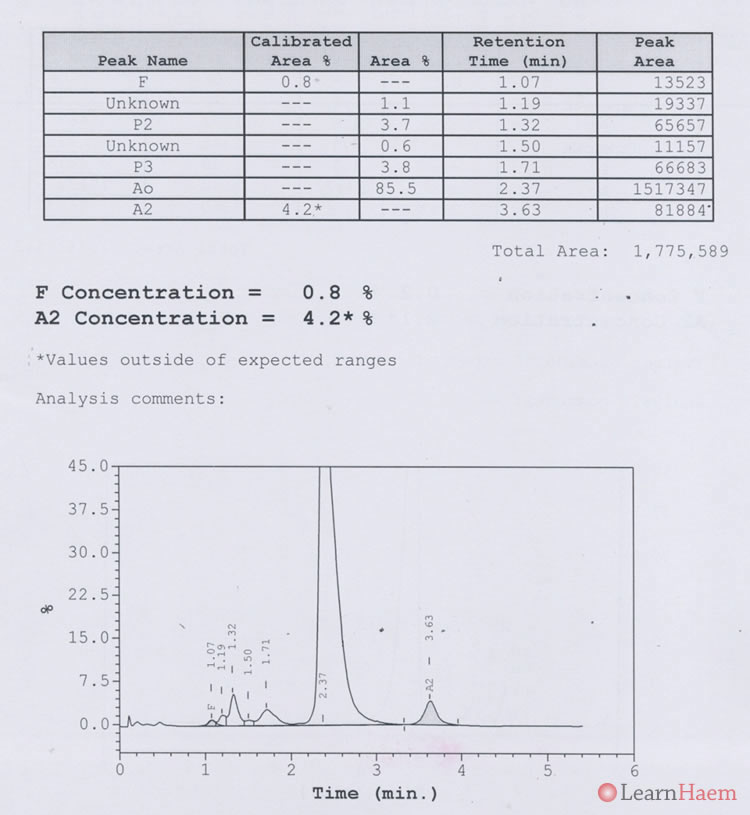
HPLC from a patient with ß thalassaemia trait. The only abnormality is a Hb A2 fraction which is above the upper limit of normal (normal range is usually 2-3.5%). In the presence of a mild microcytic anaemia in an iron-replete patient, this is highly suggestive of ß thalassaemia trait.
Other causes of a raised Hb A2:
- Anti-retroviral therapy in HIV patients
- Artifact in association with the presence of Hb S
- Hyperthyroidism
- Megaloblastic anaemia
Causes of a decreased Hb A2:
- Iron deficiency (may obscure diagnosis of ß thalassaemia trait)
- Lead poisoning
- Concomitant α thalassaemia
- Hypothyroidism
Leave A Comment