
History
- May present with:
- Blurring of vision (bitemporal hemianopia)
- Headache
- Tiredness (obstructive sleep apnoea)
- Hand numbness (carpal tunnel syndrome)
- Increased sweating
- Change in appearance
- New-onset diabetes
- Hypertension
- Symptoms of the disease
- Have you or anyone else noticed a change in your facial appearance?
- Do you have your identity card with you for reference?
- Have you noticed that you are no longer able to wear your old rings?
- Have you noticed that your shoe size has been increasing?
- Have you noticed that you or your palms are feeling more sweaty than usual?
- Symptoms of a pituitary (somatotroph) adenoma
- Have you had a persistent headache?
- Have you noticed yourself bumping into things more often than usual?
- Complications
- Increased prolactin secretion (females)
- When was the first day of your last menstrual period?
- Have you noticed that your periods have become irregular?
- Have you noticed that your periods have become unusually light?
- Have you noticed any discharge from your breasts?
- Increased prolactin secretion (males)
- Are you sexually active?
- Have you noticed any difficulty with getting or maintaining an erection?
- Cardiovascular
- Do you have a history of high blood pressure?
- Has it become more difficult to control lately?
- How many pillows do you sleep on at night?
- Do you wake up in the middle of the night feeling breathless?
- Do you get short of breath when you walk or climb a few steps?
- Have you noticed your heart beating fast or irregularly?
- Obstructive sleep apnoea
- Do you snore at night?
- Have you noticed that you are excessively sleepy in the day?
- Have you ever fallen asleep while driving?
- Gastrointestinal (colonic polyps)
- How are your bowel habits?
- Have you ever noticed any blood in your stools?
- Endocrine / metabolic
- Have you noticed that you are getting up in the middle of the night to pass urine?
- Have you noticed that you are excessively thirsty or drinking more water than usual?
- Has your diabetes become more difficult to control?
- Have you noticed that you find it unusually cold?
- Have you noticed that your voice has become hoarse?
- Musculoskeletal
- Have you noticed any pain in your joints?
- Have you noticed any tingling in your thumb or index finger?
- Do you get pain when holding a pen?
- Increased prolactin secretion (females)
Examination

{kind=link}
- General appearance
- Prognathism
- Prominent supraorbital ridges
- Coarse facial features
- Large nose and lips
- Macroglossia
- Increased teeth separation
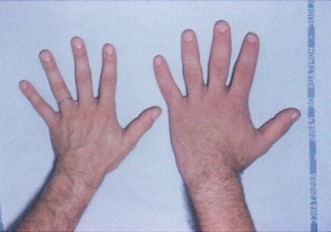
- Spade-like, doughy hands with sweaty palms
- Large feet
- May have goitre
- Visual fields – bitemporal hemianopia
- Tinnel’s test for carpal tunnel syndrome
- Examine axillae for skin tags (correlates with presence of colonic polyps) and acanthosis nigrcans
- Chest
- Gynaecomastia
- Galactorrhoea
- Cardiovascular system
- Jugular venous pulsation
- Displaced apex beat
- Lung bases for signs of pulmonary oedema
- Pitting oedema
- Joints for signs of arthropathy (e.g. Heberden’s nodes in osteoarthritis)
- Offer to examine
- Testicular volume (hypogonadism)
- Check blood pressure (hypertension)
- Urine dipstick for glycosuria
- Digital rectal examination for per rectum bleeding (colonic polyps)
Investigations
- Screening: insulin-like growth factor 1 levels should be high
- Confirm diagnosis by doing oral glucose tolerance test and showing failure of growth hormone to suppress
- Look for an underlying cause:
- Magnetic resonance imaging of the brain, looking specifically for a pituitary adenoma
- Complications:
- Fasting glucose and HbA1c to check for and assess diabetic control
- Anterior pituitary hormone screen to look for suppression from compression by adenoma
- Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) – hypogonadotropic hypogonadism (secondary hypogonadism)
- Thyroid stimulating hormone (TSH) and free T4 and T3 levels
- Adrenocorticotropic hormone (ACTH) and 8am cortisol
- Secondary adrenal insufficiency does not cause mineralocorticoid deficiency, hence salt wasting, and hyperpigmentation are not features of ACTH suppression
- Prolactin usually elevated if adenoma is a somatomammotroph
- Electrocardiogram to look for left ventricular hypertrophy and cardiac conduction abnormalities
- Transthoracic echocardiogram to assess ejection fraction
- Sleep study to look for obstructive sleep apnoea
- Consider colonoscopy as screening for colonic polyps and colonic malignancy
- Nerve conduction studies if clinically suspect carpal tunnel syndrome
Management
- Multidisciplinary approach
- Patient education, advice not to drive if having visual symptoms
- PT/OT if functionally affected
- Treat the underlying cause
- Surgery: trans-sphenoidal resection of the pituitary adenoma (cure rate better for microadenomas)
- Medical: traditionally if surgery has failed or is not possible
- Somatotropin receptor ligands (octreotide and lanreotide) – suppress GH and IGF1 levels effectively and safely; also improves most clinical manifestations of acromegaly
- Growth hormone receptor antagonists (pegvisomant) as second-line
- Treat complications
- Continuous positive airways pressure for obstructive sleep apnoea
- Diuretics, ACE inhibitors, beta blockers for congestive cardiac failure
- Hypoglycaemic agents for glycaemic control
- Replace hormones if anterior pituitary screen shows deficiency
Summary
Sir, this patient presents with an insidious history of increasing sweatiness, tiredness and change in appearance. The most likely diagnosis is acromegaly. On examination, there is a bitemporal hemianopia, suggesting a pituitary adenoma as an underlying cause. There is prognathism, increased dental separation, macroglossia as well as increased palm and sole size.
Regarding complications, the patient reports excessive daytime sleepiness, which leads me to wonder if there is an element of obstructive sleep apnoea. The apex beat is not displaced, and there is no evidence of congestive cardiac failure. There is nothing in the history to suggest diabetes mellitus, an arthritis or carpal tunnel syndrome complicating the disease.
I would like to confirm my diagnosis by demonstrating a failure of growth hormone suppression in response to an oral glucose load. Further investigations would be directed at looking for an underlying cause, such as magnetic resonance imaging to look for a pituitary adenoma. In terms of complications, I would like to obtain a fasting blood glucose and HbA1c level to look for evidence of diabetes. I would also like to do an anterior pituitary hormone screen to rule out hormonal suppression from tumour compression. An electrocardiogram would be useful to screen for left ventricular hypertrophy and cardiac conduction abnormalities, and a sleep study to confirm obstructive sleep apnoea.
In summary, this patient has acromegaly.
Leave A Comment