
Mixed-phenotype acute leukemias are rare acute leukemias that has an ambiguous pattern of antigen expression. This may constitute a population of blast with multiple antigens of different lineages expressed on the same cell (biphenotype) or different population each expressing antigen of a different lineage (bilineage). MPAL generally have a poor prognosis.
Diagnostic Criteria (WHO 2016)
The diagnosis of mixed phenotype acute leukaemia relies on immunophenotyping. Requirements for lineage assignment include:
1) Myeloid Lineage
- MPO (by flow cytometry, immunohistochemistry, or cytochemistry) or
- Monocytic differentiation (≥ 2 of the following: non-specific esterase, CD11c, CD14, CD64 or lysozyme)
2) T-cell lineage
- Cytoplasmic CD3 (by flow cytometry with antibodies to CD3 epsilon chain. Immunohistochemistry using polyclonal anti-CD3 antibody may detect CD3 zeta chain, which is not T-cell-specific) or
- Surface CD3 (rare in mixed-phenotype acute leukaemias)
3) B-cell lineage (multiple antigens required)
- Strong CD19 with ≥1 of the following strongly expressed: CD79a, cytoplasmic CD22, CD10 or
- Weak CD19 with ≥2 of the following strongly expressed: CD79a, cytoplasmic CD22, CD10


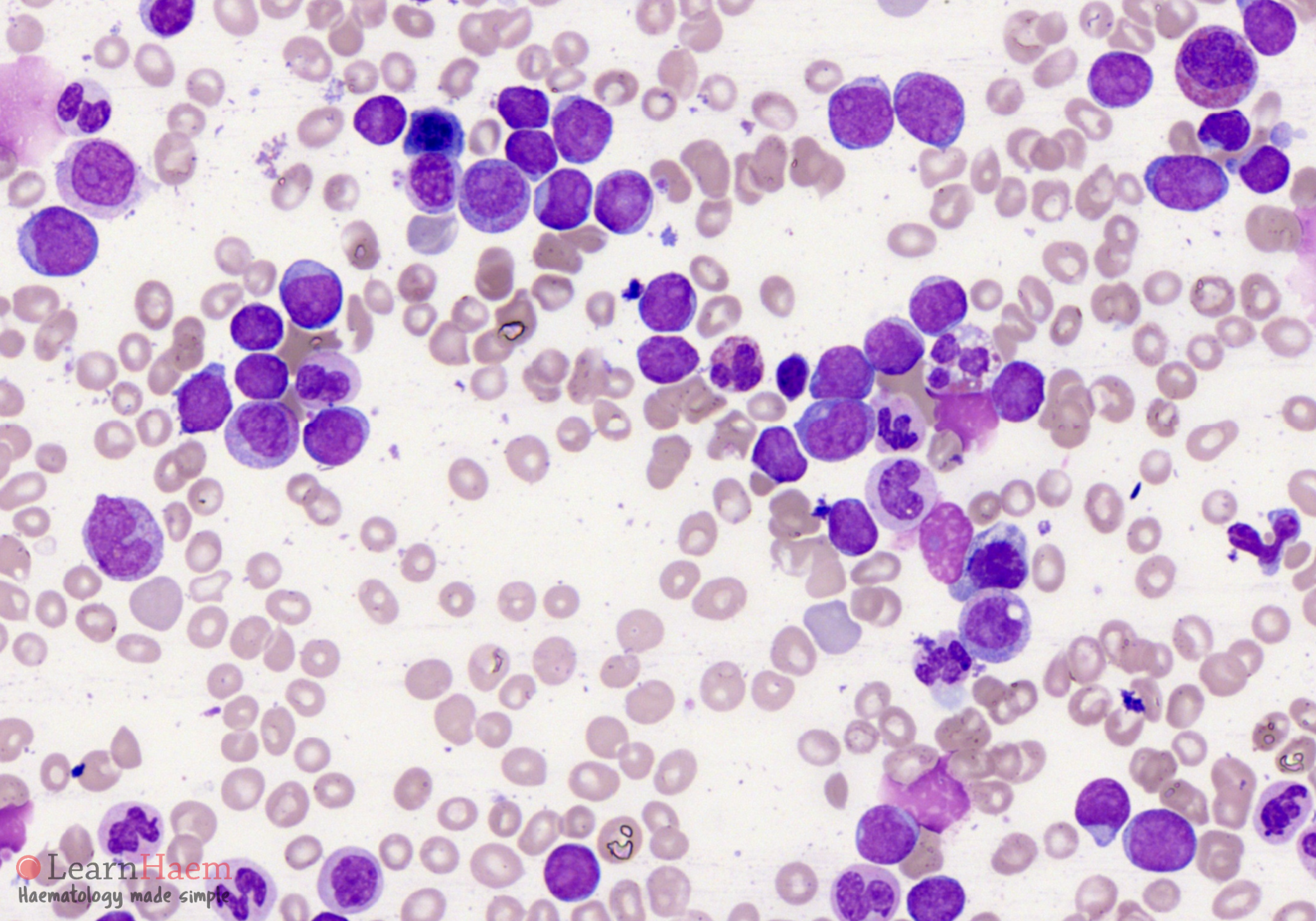
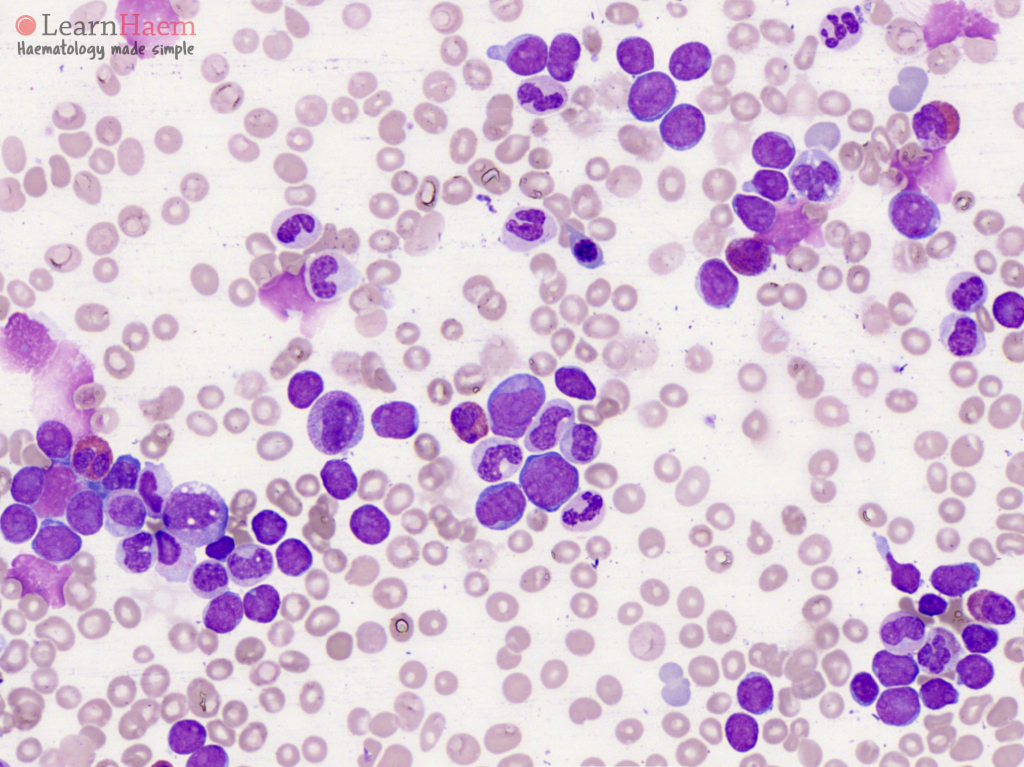
Peripheral blood films from two patients with mixed phenotype acute leukemia. There are a significant number of circulating blasts. Most are morphologically lymphoblasts but there is a separate population of larger blasts which are more myeloid in appearance. Correlation with immunophenotyping is required for diagnosis.
Blood Film Features:
- Blast features may be undifferentiated or dimorphic
- Undifferentiated blast population: no morphologically differentiated features
- Dimorphic blast population: some blasts resembling myeloblasts or monoblasts and some resembling lymphoblasts
Bone marrow aspirates from two patients with mixed phenotype acute leukaemia.
Bone Marrow Features:
- Blast population: as described above
- Cytochemistry: MPO or non-specific esterase to delineate myeloid lineage
Leave A Comment