
Burkitt lymphoma (BL) is a highly aggressive lymphoma, usually associated with a MYC translocation to an immunoglobulin locus, with three distinct epidemiological variants:
- Endemic BL: mainly in equatorial Africa and Papua New Guinea, usually presenting as a childhood malignancy with head and neck tumours. More common in males, thought to be driven by Epstein-Barr virus (EBV) or Plasmodium falciparum.
- Sporadic BL: occurs in both children and adults, more common in males. Typically presents aggressively with abdominal masses and ascites. Head and neck involvement is rare. Sporadic BL is not as commonly associated with EBV.
- Immunodeficiency-associated BL: this most commonly occurs in the setting of human immunodeficiency virus (HIV) infection. It typically manifests when the CD4+ count is still normal or low-normal. Nodal and bone marrow involvement are common. Despite this, it is considered an AIDS-defining disease as it can EBV-driven in the setting of immunodeficiency.
Due to its highly aggressive nature, BL patients may present with spontaneous tumour lysis and acute kidney injury. CNS involvement may be seen at diagnosis or early in the disease course.
Differential diagnosis
- Acute lymphoid leukaemia
- Blastoid mantle cell lymphoma
- Diffuse large B cell lymphoma
Burkitt Lymphoma vs DLBCL
Differentiating Burkitt lymphoma from DLBCL is important as studies have shown that BL outcomes when treated with conventional R-CHOP chemotherapy are poor. In addition, BL has a higher risk of CNS involvement compared with standard DLBCL. Features which may help differentiate BL from DLBCL include (Bellan et al., 2009):
- Biopsy of bone marrow or lymph node to demonstrate monotonous infiltrate of medium-sized atypical lymphoid cells.
- Immunohistochemistry: BL arises from a germinal centre B cell and is almost always BCL2 negative. The typical immunophenotype is: CD20+/10+/Bcl6+/Bcl2-/myc+
- Simple cytogenetics with myc translocation – t(8;14) most common, but light chain translocations also seen: t(2; 8). t(8;22). In contrast DLBCL often has complex cytogenetic abnormalities.
- There are a high proportion of mitotic figures due to the aggressive nature of the disease. Ki-67 100%. This is the least specific as DLBCL may also have an extremely high Ki-67 index.
Peripheral Blood Features


0 x
- Circulating Burkitt lymphoma cells may be seen
- Leukoerythroblastic picture and teardrop cells may be indicative of underlying marrow infiltration.
Bone Marrow Features
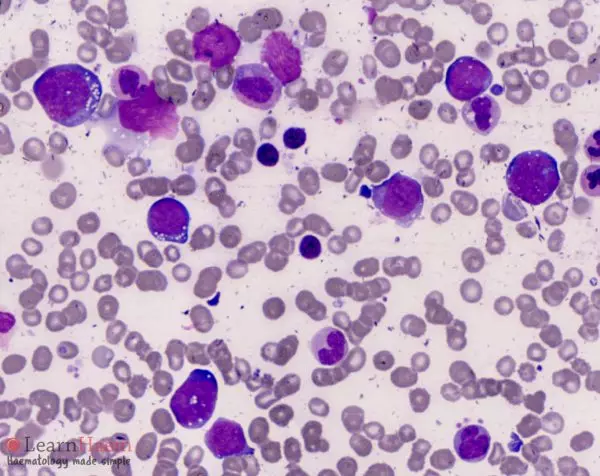
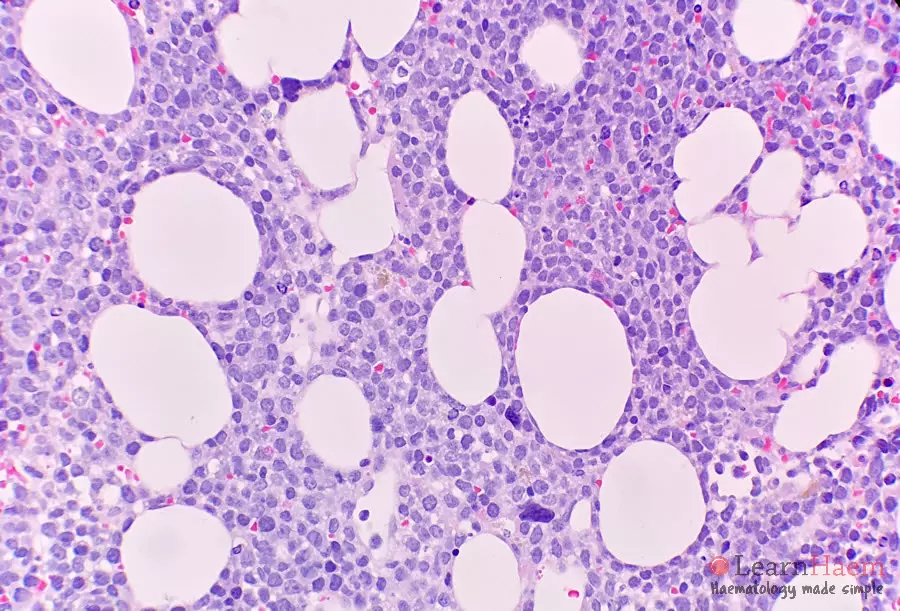
- Medium-sized, monotonous atypical lymphoid cells
- Deeply basophilic cytoplasm
- Cytoplasm often vacuolated
- Nuclei characterised by mildly clumped chromatin, often with multiple nucleoli
- Starry sky pattern on histology specimens is due to abundance of macrophages taking up apoptotic cells
0 x
0 x
Leave A Comment