
Haemophagocytic lymphohistiocytosis (HLH) describe a spectrum of primary and secondary disorders characterised by uncontrolled macrophage activation and haemophagocytosis of haematopoietic cells. Familial cases present early in childhood, and are usually due to mutations in the perforin gene, though other genes have also been identified. Secondary causes of HLH include:
- Malignancy, typically aggressive lymphomas
- Infections:
- Viral (cytomegalovirus, herpesviruses, adenoviruses etc.)
- Bacteria, especially Mycobacterium tuberculosis
- Rarely, fungi such as in disseminated histoplasmosis, or other parasitic infections
- Autoimmune disease
- Drugs
Diagnostic Criteria
The following diagnostic criteria have been applied to HLH, but it is important to note that they are not specific for HLH and that some of the tests may not be widely available. In addition, they do not take into account some of the typical presenting features such as transaminitis or jaundice.
- Fever ≥38°C
- Splenomegaly
- Peripheral blood cytopaenias:
- Hb <9g/dL
- Platelets <100×109/L
- Absolute neutrophil count <1×109/L
- Hypertriglyceridaemia (fasting triglycerides >265mg/dL) or hypofibrinogenaemia (fibrinogen <1.5g/L)
- Haemophagocytic activity in the bone marrow, spleen, lymph node or liver
- Raised ferritin of >500ng/mL (although levels >3000ng/mL may be more suggestive)
- Low or absent NK activity
- Elevated soluble CD25
- Elevated CXCL9
Peripheral Blood Features


The patient is often cytopaenic (see criteria above). Patients with bone marrow infiltration may have teardrop cells or a leukoerythroblastic picture.
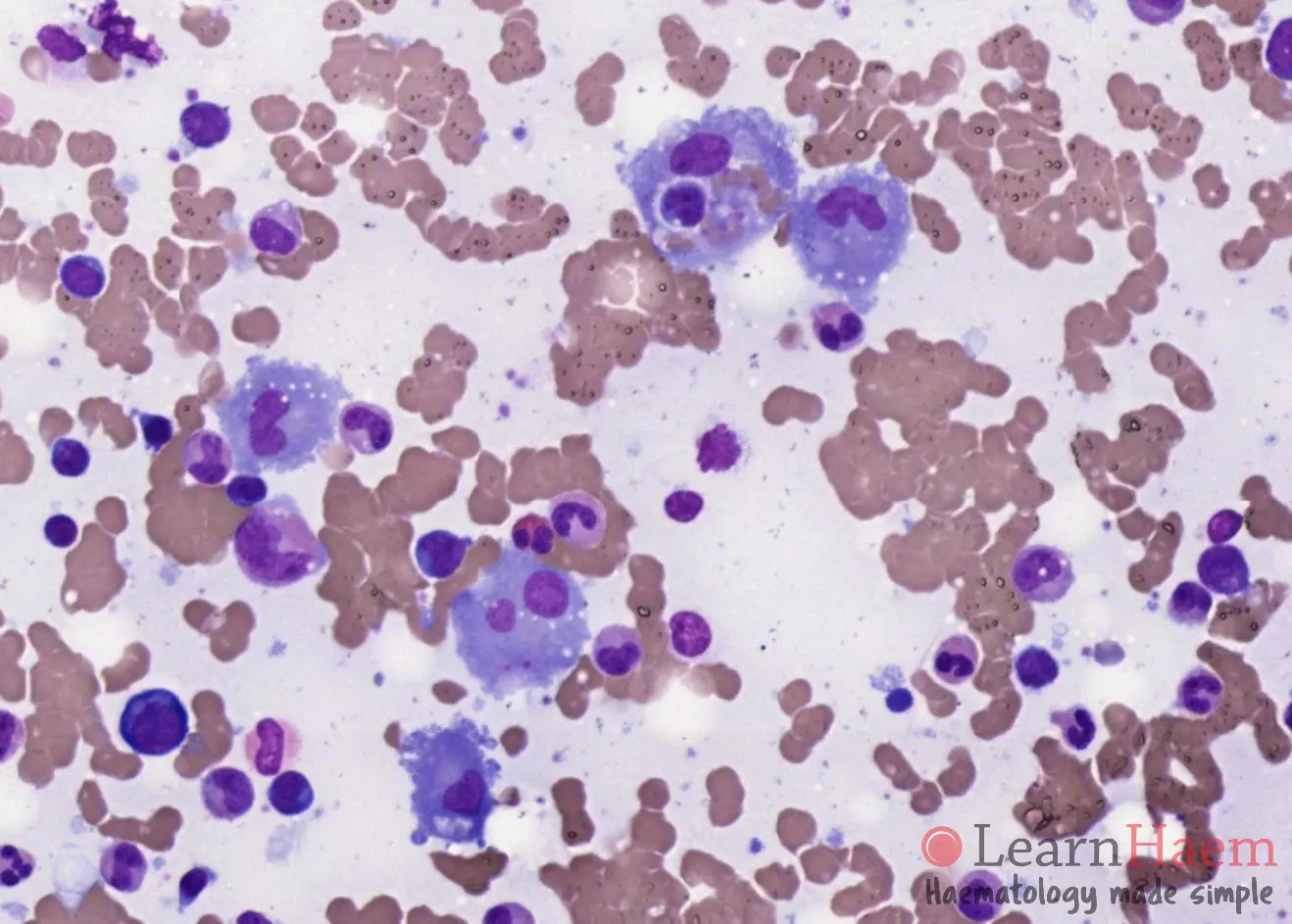
Bone Marrow Features
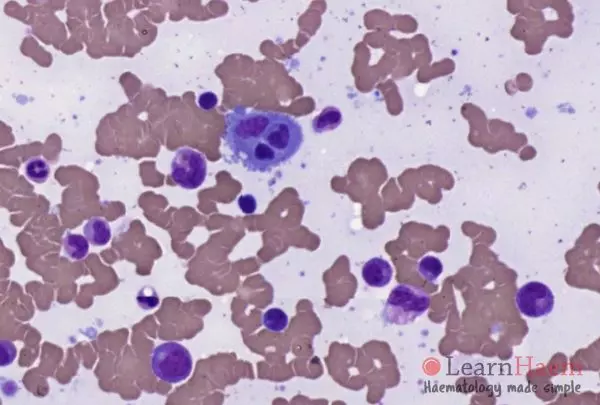
- Increased histiocytic activity
- Histiocytes with active haemophagocytosis have recognisable haematopoietic cells in their cytoplasm. This should be distinguished from cellular debris which can be seen in reactive bone marrow aspirates.
- Atypical lymphoid cells should be actively sought, as they may provide an underlying cause (lymphoma) for the HLH. The last three slides are from patients with HLH secondary to DLBCL (slides 2 and 3) and a T cell lymphoma (slide 4).
Leave A Comment