
Chronic myelomonocytic leukaemia is a chronic leukaemia with both proliferative and dysplastic features. It is classified based on the peripheral and bone marrow blast percentage. Prognosis for CMML is generally poor and allogenic haematopoietic cell transplantation is the only curative therapeutic option at the moment.
Diagnostic Criteria (WHO 2016)
- Persistent peripheral blood monocytosis (≥ 1 x 109/L), with monocytes accounting for ≥10% of the leukocytes
- WHO criteria for BCR-ABL1-positive chronic myeloid leukaemia, primary myelofibrosis, polycythaemia vera and essential thrombocythemia are not met.
- No rearrangement of PDGFRA, PDGFRB, FGFR1 or PCM1-JAK2 (which should be specifically excluded in cases with eosinophilia).
- Blasts constitute <20% of the cells in the peripheral blood and bone marrow
- Dysplasia involving ≥1 myeloid lineages; or if myelodysplasia is absent or minimal, criteria 1―4 are met and:
- An acquired, clonal cytogenetic or molecular genetic abnormality is present in haematopoietic cells; or
- The monocytosis has persisted for ≥3 months and all other causes of monocytosis (e.g. malignancy, infection, and inflammation) have been excluded.
Classification (WHO 2016)
- CMML-0: < 2% blasts in the blood and < 5% in the bone marrow, and no Auer rods.
- CMML-1: 2-4% blasts in the blood or 5-9% in the bone marrow, and no Auer rods.
- CMML-2: 5-19% blasts in the blood, 10- 19% in the bone marrow or Auer rods are present


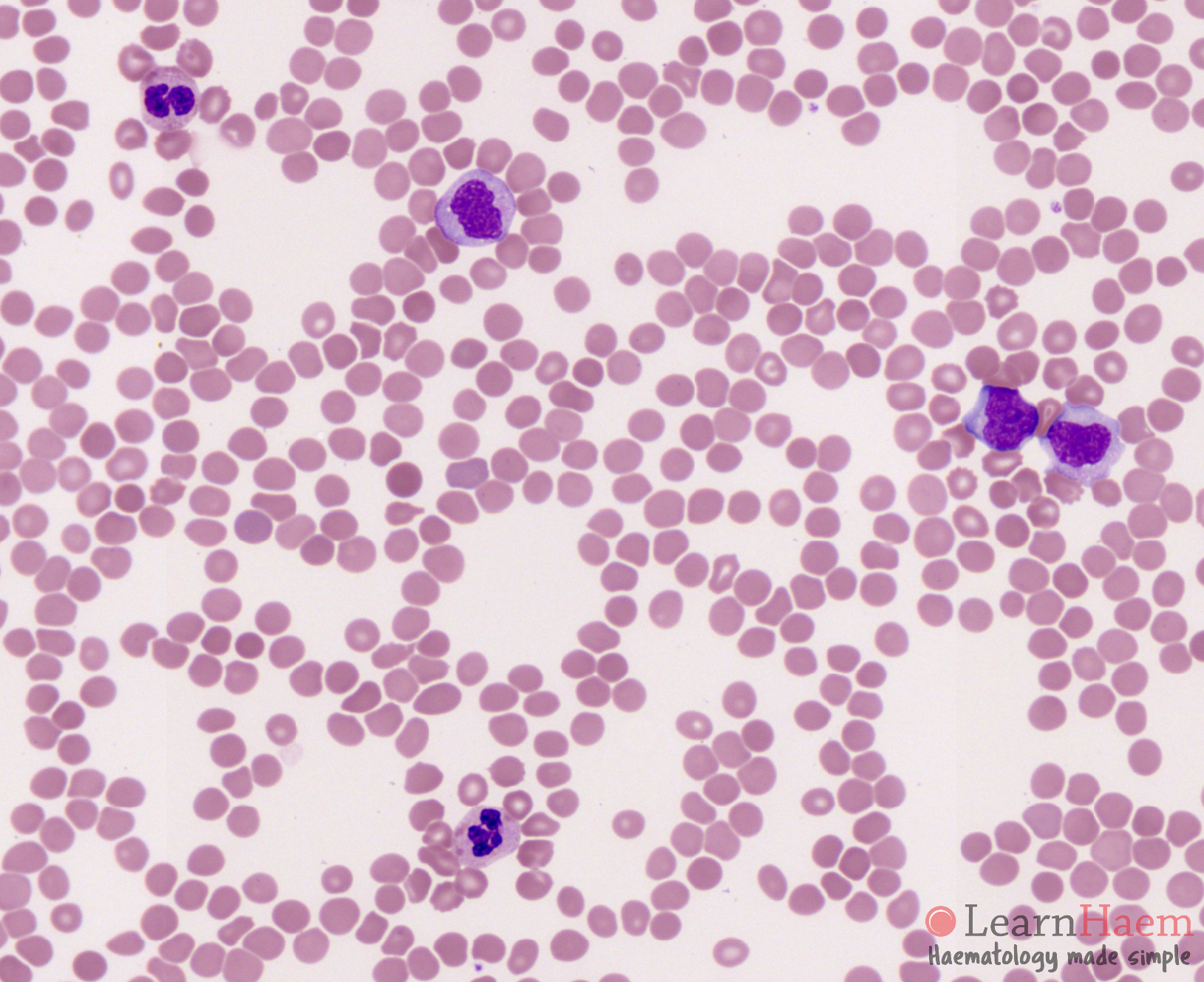
Peripheral blood film of a patient with CMML-0.
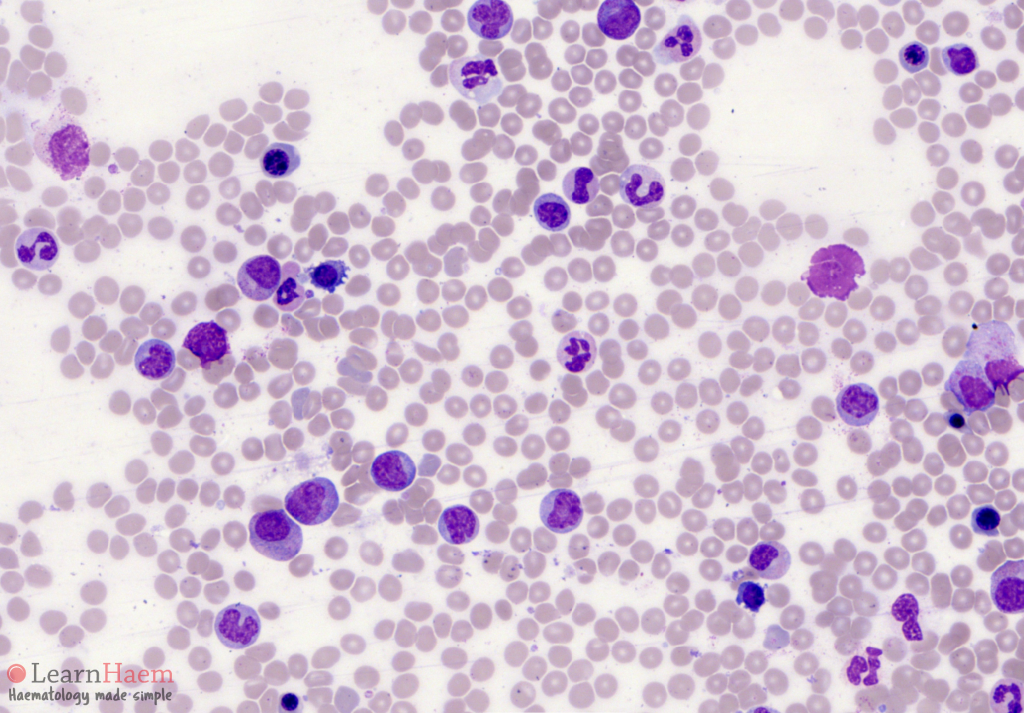
Peripheral blood film of a patient with CMML-2. Note the monocytosis and presence of dysplastic neutrophils.
Blood Film Features:
- Monocytosis (> 10% of leucocytes, with an absolute count ≥ 1 x 109/L): usually mature, may have some abnormal nuclear segmentation and granulation
- Dysplasia: predominantly dysgranulopoiesis (see MDS overview page for specific features)
- < 20% Blast: include myeloblast, monoblast and promonocytes in the calculation of the blast percentage
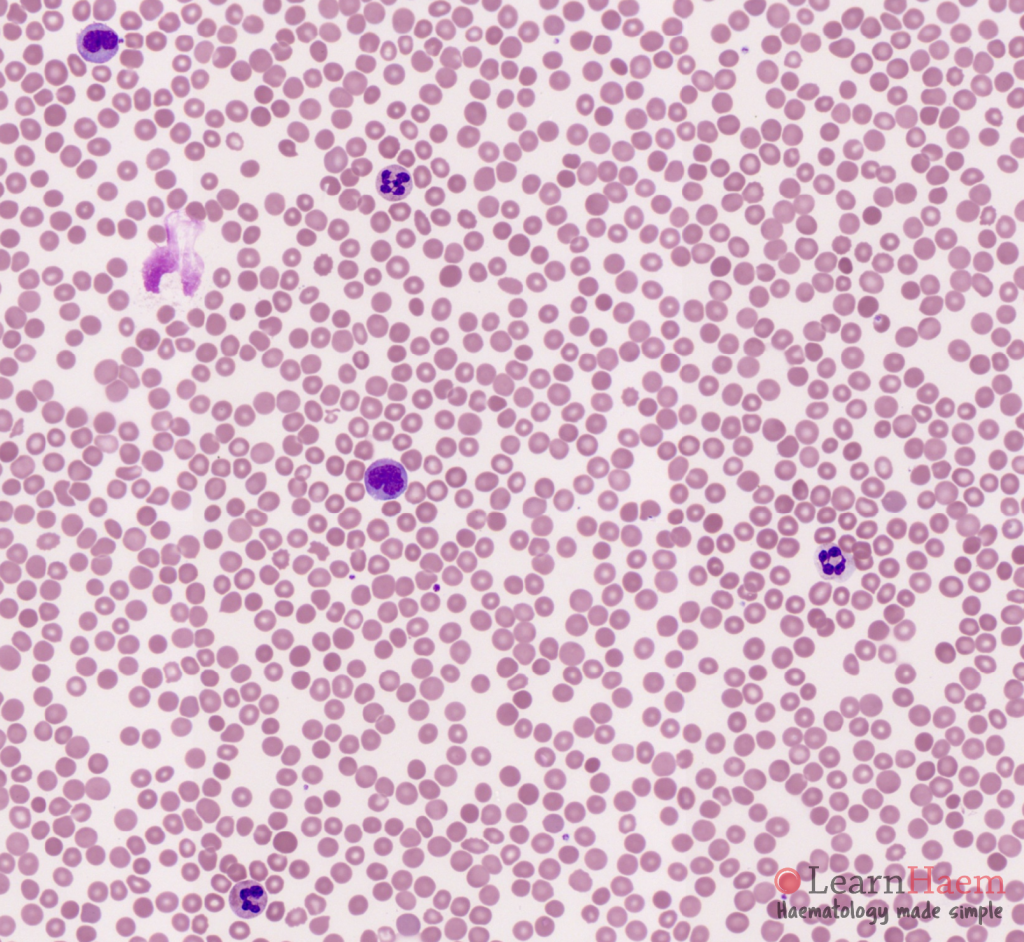
Peripheral blood film of a patient with CMML on hydroxyurea treatment.
Other features to look for:
- Hydroxyurea therapy: macrocytosis, stomatocytes, hypersegmented neutrophils
Bone marrow aspirate from a patient with CMML-0.
Bone marrow aspirate from a patient with CMML-2. Note the marked hypercellular marrow with presence of myeloblasts, monoblasts and promonocytes. As these account for <20% of the total nucleated cell count, the diagnosis is CMML (as opposed to acute myelomonocytic leukaemia).
Bone marrow aspirate from a patient with CMML with plasmacytoid dendritic cells. Note the presence of surrounding plasmacytoid dendritic cells are identified by their basophilic cytoplasm and eccentric nuclei. They may have cytoplasmic projections, and precipitates of immunoglobulin.
Bone Marrow Features:
- Hypercellular marrow
- Myeloid:Erythroid (M:E) ratio increased
- Increased monocytic population
- Dysplasia: predominantly dysgranulopoiesis, look for dyserythropoiesis and dysmegakaryopoiesis as well (see MDS page for specific features)
- < 20% blasts: include myeloblast, monoblast and promonocytes in the blast enumeration
- Cytochemistry: alpha-naphthyl acetate esterase (with fluoride inhibition)
Differentials Diagnosis:
- Acute myeloid leukemia: may transform from underlying CMML or de novo AML (M4/5) with underlying dysplastic changes
- Myelodysplastic syndrome: less prominent monocytosis, may have more prominent dysplasia
- Atypical chronic myeloid leukaemia: predominantly myeloid proliferation, less prominent monocytosis, will also have dysplasia
Leave A Comment