
Acute lymphoblastic leukaemia (ALL) occurs when there is a malignant proliferation of B or T lymphoid progenitors. Blasts are small with a high nuclear-cytoplasmic ratio. It is the most common form of leukaemia in children, accounting for >80% of childhood leukaemias. It is rarer in adults, comprising <20% of adult leukaemias.
Malignant proliferation may be intra-medullary or extra-medullary. The distinction is arbitrary, as both are treated in the same way. By convention, if bone marrow blasts exceed 25%, the diagnosis is ALL, regardless of whether there are extra-medullary lesions. If a patient has extra-medullary lesions comprising lymphoblasts but a bone marrow blast of <25%, they are classified as having lymphoblastic lymphoma (LBL). Unlike in AML, there is no agreed-upon lower limit for the blast percentage required for the diagnosis of ALL.
Note that presentation with a mediastinal mass is one of the classic presentations of T-LBL. This is the reason that the peripheral blood film must be carefully examined in all patients presenting with a mediastinal mass.
Lineage Assignment
The WHO has clear criteria for lineage assignment. These are illustrated in the table below. The criteria are important as blasts of T and myeloid lineage may aberrantly express CD19, incorrectly leading to a diagnosis of mixed phenotype acute leukaemia (MPAL).
| Lineage | Criteria |
|---|---|
| Myeloid | MPO expression; or Expression of monocytic markers (≥ 2 ofnon-specific esterase, CD11c, CD14, CD64 or lysozyme) |
| B | Strong CD19 with ≥1 of CD79a, CD22 or CD10 strongly expressed; or Weak CD19 with ≥2 of CD79a, CD22 or CD10 strongly expressed |
| T | Cytoplasmic or surface CD3 by flow cytometry. CD3 staining by IHC may detect the CD3 zeta chain, which is not T cell specific and can also be seen on NK cells. |
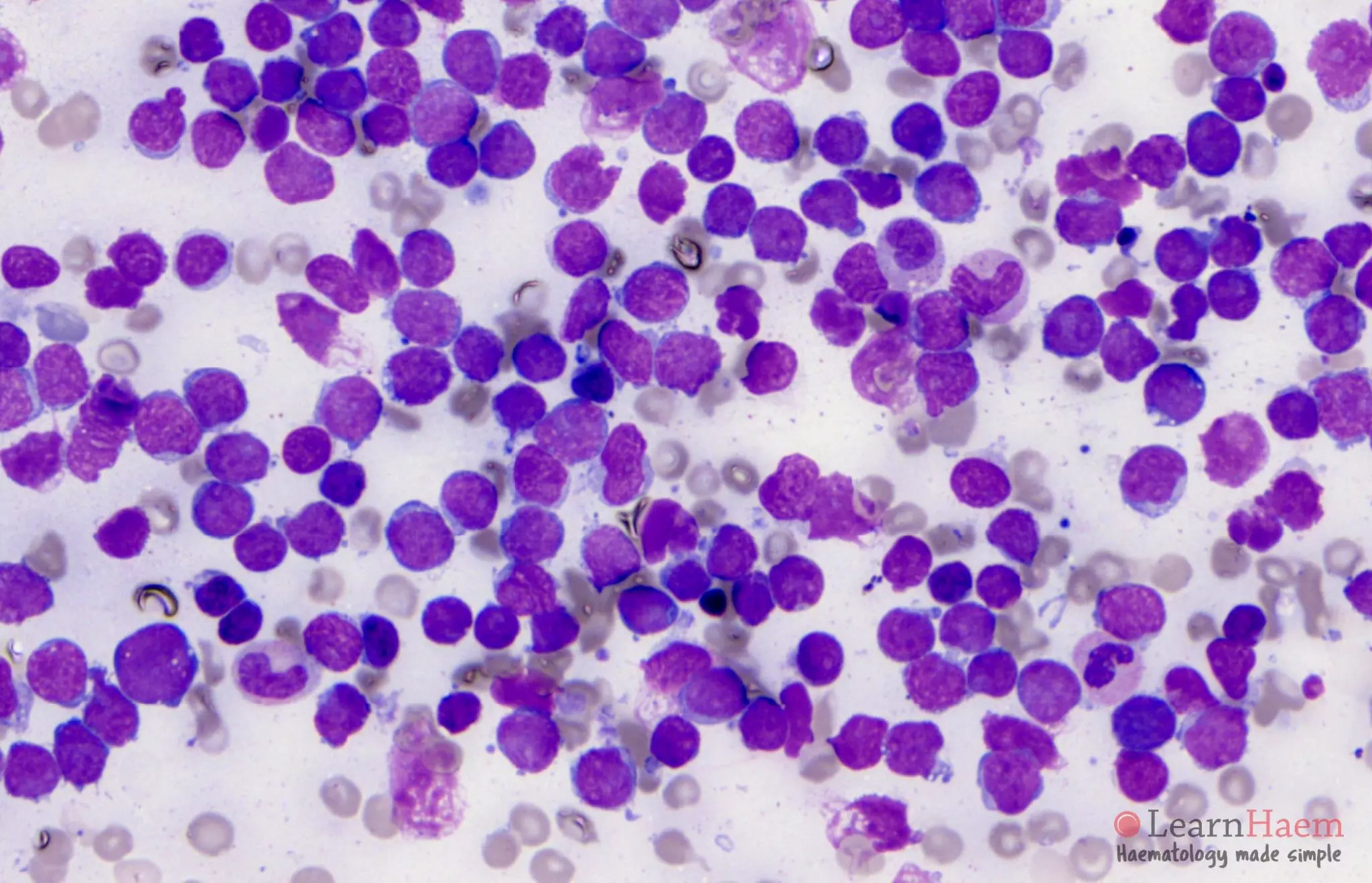
Peripheral Blood Features


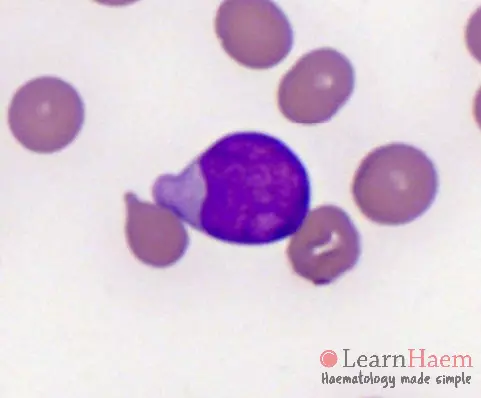
- High nuclear : cytoplasmic ratio.
- Agranular, weakly basophilic cytoplasm.
- Absence of Auer rods.
- Regular, round cytoplasmic and nuclear outline.
- Inconspicuous nucleoli.
- The first slide in the series above shows classical ALL blasts in the peripheral blood.
- L2 lymphoblasts may be larger and more pleomorphic. Similarly, T lymphoblasts tend to have more irregular nuclear shapes (slides 3 and 4 above).
- Background RBCs, WBCs and platelets should not have morphological dysplasia.
Bone Marrow Features
- Hypercellular marrow.
- Marrow is typically near-completely replaced by lymphoblasts.
- Very little normal haematopoiesis.
- Dysplastic features are typically absent, in contrast to AML.
Leave A Comment